
Official websites use .gov
A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you’ve safely connected to the .gov website. Share sensitive information only on official, secure websites.
Taking Measure
Just a Standard Blog

For as long as we have had automobiles, we have had traffic accidents. Even the vehicles that we depend on to take care of us in the event of an accident—ambulances—get into accidents nearly every day. Because ambulances are basically a small emergency room on wheels, the occupants in the back are at perhaps even more serious risk of being injured or killed during an accident than those in other vehicles. This is especially true when you consider that ambulances are often weaving through traffic at high speed on the way to the hospital.
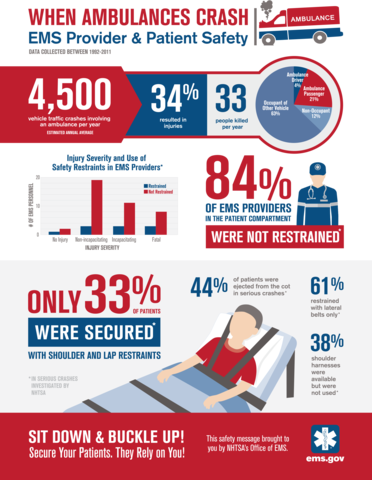
According to a 20-year National Highway Traffic Safety Administration (NHTSA) study (PDF), there is an average of 4,500 crashes involving ambulances every year. Of those crashes, the report found that 84 percent of emergency medical service (EMS) providers in the patient compartment were not wearing a seat belt or some other restraint. The report also found that 44 percent of patients were ejected from the cot in serious crashes.
Obviously, this raises a number of very serious safety concerns for providers and patients.
If you’re lucky enough to have never seen the inside an ambulance, let me give you a general idea of what you would see. There is a cot, usually a bench seat on the side closest to the curb, a bucket seat at the head of the cot and sometimes a seat on the side closest to the street. There are communication devices and medical equipment, e.g. cardiac monitors, oxygen, and suction machines, cabinets filled with supplies, and needle and trash disposal bins.

When I look at today’s ambulances, what I see is equipment not properly stowed or mounted, slippery floor surfaces, open cabinet doors, lots and lots of sharp edges, and, most importantly, seating arrangements that do not allow medical personnel to reach both their patients and the supplies they need while seated. Providers feel they have no other option but to stand up and walk around inside the compartment while racing down the highway. Would you want to be standing in your car while moving through traffic at highway speeds?
I know I wouldn’t, and unless you’re some kind of daredevil, I doubt you would either.
Fortunately, this is where standards can have a huge impact on safety and people’s lives—YAY standards!
Over the past several years, federal, state and local agencies, trade organizations, manufacturers, and numerous EMS professional organizations came together to develop consensus-based ground automotive ambulance standards. These standards are based on both test methods for crash testing and design elements to make the inside of the compartment more user-friendly and safe.
In March, the Commission on Accreditation of Ambulance Services (CAAS) released their Ground Vehicle Standard (GVS v.1.0) for automotive ambulances, and last fall the National Fire Protection Association (NFPA) released NFPA 1917, 2016 edition Standard for Automotive Ambulances. These standards incorporate the Department of Homeland Security (DHS)-sponsored work from NIST and the National Institute for Occupational Health and Safety (NIOSH) as well as many test methods that have been developed by the National Truck and Equipment Associations Ambulance Manufacturers Division and the Society of Automotive Engineers.
Now let me explain how we got there.
The EMS community had long felt that there needed to be a more rational, scientific approach to ambulance design. After all, there had been little significant change since the 1970s when the EMS community was just beginning to move away from using hearses. Save that piece of trivia for your next dinner party!
Also, because of their size, ambulances did not need to meet most of the same crash testing requirements that apply to our cars. They actually fall in the same category as those shuttle buses at the airport—when was the last time you wore a seat belt in one of those?
The crash-test work NIOSH did in the early 2000s really laid the foundation that we built upon. They conducted four full-vehicle crashes to look at how worker restraints performed, but the testing also revealed other areas of concern related to cot mount strength, seat belt location and seat strength, cabinet location (head impact risk) and lack of equipment mounting.
The good news is that this early testing really helped the ambulance industry better understand the need for standards.
From 2010-2015, NIOSH partnered with the ambulance manufacturing community to conduct crash tests of entire ambulances, cots, seats, cabinets, and equipment mounts. The community voluntarily supplied and paid for all the parts (cots, seats, cabinets) NIOSH needed for testing. During this time, the partners crafted new test procedures that work for ambulances while manufacturers tried new designs. Now, the community tests the components and vehicles on their own using the same pass/fail criteria and equipment that the NHTSA uses to ensure our vehicles are safe to drive.
Seeing an entire industry become so involved in the standards development and conformity process like this is really gratifying. It makes me feel good about what I do, and we have better products on the market today because of it.
With a solid foundation in place, we turned our attention to the inside of the compartment. We took many of the issues the community identified during research and approached them with “human factors” in mind. Human factors is concerned with understanding how humans interact with their surrounding system—in this case how EMS providers interact with their patients and the workspace in the patient compartment. Based upon the information collected, we developed over 200 individual criteria that focused on improving seating and restraints, workspace, communications, storage and other areas.

With a team of computer scientists, systems engineers, human factors experts, and a DHS contractor, we developed several new designs for patient compartments. We then loaded the designs into simulation software so we could apply different emergency scenarios (e.g., cardiac arrest, trauma, etc.) and see if a provider could do everything they needed to do to provide care while remaining seated and restrained.
After we finished with that, we worked with NFPA and CAAS to make sure that they were incorporating human factors into their standards—things like how best to position the cot, equipment, cabinets, and needle disposal so that they were all within arms-reach of the EMS provider, and they are defining what is in “arms-reach” in terms of where the majority of care will take place—the primary patient care position—where the EMS provider sits.
We also pushed for recessed overhead lighting and handlebar requirements and for clearance space around the provider’s head to limit the chances for severe head trauma. And lastly, as a complement to the standards, we worked with DHS and their contractor to develop the Ambulance Patient Compartment Human Factors Design Guidebook (PDF), which serves as a starting point for the design of a new ambulances and contains best practices for human factors and ergonomics such lighting, climate control and communication.
Ambulances save lives every day, but too many lives are lost when ambulances get into accidents. Our number one goal with this project was to keep EMS providers seated and restrained so that they can work to save their patients’ lives without having to risk their own.
I’m proud of what we’ve accomplished. I have no doubt that these standards will keep both our brave EMS providers and their patients safer in the future.
About the author

Related Posts



Comments
- Reply
Thank you
These new safety standards for ambulances benefit both the patients being transported and the paramedics alike. Ambulance accidents can be some of the most devastating accidents, everything from collisions with distracted drivers unaware of emergency vehicles like an ambulance, to crashes with intoxicated motorists who later have to fightDUIcharges in court.
Hopefully under these new safety measures for ambulances, they will protect a patient's injurylawrights while being medically transported, along with helping EMTs be safe on the job while performing their essential life saving care.
You can change everything about the Ambulance. The change needs to be in The Control of Human mistakes. That human factor without mandating controls as has the trucking industry and Federal Aviation industry. The one focus no one wants to change. How to stop Fatigue. The ambulance drivers are driving 24, 36, 48, and more hours while on shift without rest. Counties in Ga. A Paramedic works 24hrs in one county, gets off and goes to the next county without rest. No policies on rest. No policies on maximum duty hours. No policies on maximum duty hours limited per day. No policies for mandatory "Rest" before working. All the Date shows this is the problem. No one wants to change. In the safety world this is known as "The Challenger Effect", "Drift", and or "Naturalization of Deviation".
Protect the Ambulance by protecting the people who drive them and the people they will injure when the drivers are fatigued.